
domain:youtube.com?page=1?page=2

It's designed well, people just refuse to use it correctly and we can't force them.
"People refuse to use it correctly" sure looks like bad design from the outside.
Ever heard of "Desire paths?". You can have a beautifully engineered and designed walkway, and people will still walk through the dirt if that makes more sense to them.
Similarly, you can try to get people to use their PCP as the doorway... but if that's too complex or annoying of a process they'll skip that and use urgent care.
Maybe just maybe there's a way that accommodates people's preferences.
 Terracotta
10hr ago
Terracotta
10hr ago
Most people are aware of Bipolar disorder, at least superficially. Lots of people say "I have mood swings" and tell that to healthcare workers with less training, these people dutifully write down Bipolar in the chart. Or they say "you ever like have mood swings and be unable to sleep?" Gets the diagnosis. Someone who actually has Bipolar 1 with a manic episode barely sleeps for a week of more, does illegal things, or spends ALL of their money in the bank account and all kinds of other stuff. The diagnosis is serious and life limiting without treatment. The medications are also serious - most patients get antipsychotics these days which increase all cause mortality. They are worth it if you actually have the disease. Put undertrained staff give the dx to people who don't have it and then suddenly...
OK, this is a good example for illustrating the difficulty I'm having with the binary MD-competent/ NP-incompetent model. So here we have a fairly clear, potentially dangerous error in practice. Insofar as it is fairly clear, you were able to explain it to me in a paragraph or so: now I, a random Mottizen, understand that it's bad to diagnose and medicate bipolar just on the basis of "mood swings" or "poor sleep," and that patients should instead be experiencing very florid manic episodes with clear life consequences. That's facile, but for someone going on to psych practice, I'd imagine a few additional hours of video case studies would eliminate the lowest-hanging 80-90% of obvious mistakes of the form "don't diagnose bipolar in this clearly not-bipolar patient, dummy." So presumably that same advice and video training could be administered to a DNP before they begin psych practice, problem solved.
Fine, says the MD, but what about the top-10% "art of medicine" situations where the line is far more nuanced? There aren't empirical tests to verify a diagnosis; what if the situation sounds right on the border? The precise mechanisms of bipolar are poorly understood; what if there are a lot of other things going on and it's not clear how they interact? Or it's not clear how medication will impact any particular patient, so what if the risk-benefit math around prescription is very challenging?
I can easily see how what you call the "skill ceiling" could come into play there, leading an NP to get those questions wrong. What I don't see is the training value-add that makes you confident a random board-certified psychiatrist would clear the skill ceiling and get them right. There's not good basic science around these issues, so the organic chemistry and anatomy from med school certainly won't help. Residency? Presumably this means that the MD encountered some difficult cases under supervision and was admonished to approach each case the way their attending would do it. However, (a) that could have been an indefinite amount of time ago, and there's nothing beyond some trivial online quizzes to ensure the MD has kept up with new data since their training; and (b) even back in training, nobody was checking to make sure the supervisor was themselves particularly judging the situation "correctly". Indeed, how could anyone even define "correctly," if the case was by definition so difficult and subtle, the kind of situation where the wrong call would just make a patient sadder and less functional 20 years hence, not cause them to keel over and die on the spot? Doubtless the attending felt confident that their approach was making a real difference; but we all know the various cognitive biases that would lead doctors to overestimate the correctness of their judgment and the effectiveness of their treatment under those circumstances.
I guess it boils down to the broader question "when psychiatry works clearly, it should work for DNPs too; but when it doesn't work clearly, how can you be sure it works at all?" One established answer is to turn to empirical investigation to discipline our judgment; but as you point out, psychiatry isn't a field with a lot of options for carefully blinded RCTs and massive long-term studies.
anti_dan
10hr ago
Legacy media is left wing. New media isn't conventionally left or right, but the most popular versions tend to lean republican.
These are related. Just like how Fox News was the biggest cable news channel, despite being a drop in the bucket overall. They were the only people putting out a product lots of people wanted. In addition to that effect, the current crop of left wing views cannot sustain themselves in a questioning environment. Joe Rogan and the podcast sphere didn't start on the right, they slowly walked there because that is what happens outside of the left wing censorship regime.
FirmWeird
Randomly Generated Reddit Username
10hr ago
As the 2024 election is mulled over by pundits to see what, exactly, went wrong, I wonder if we are missing similar “warning signs” in trends. The Bernie-Bro-turned-Trump-supporter pipeline a la Joe Rogan could be symptomatic of voters aligning more along an axis of “insiders vs. outsiders” instead of policy preferences, education, age, or race; while there are correlations with each of those things to an “insiders vs. outsiders” axis, none of them are definitive.
I'm on the record as saying that this has been coming for quite a while now. Google is broken and not finding my posts on the old subreddit, but I said this 10 months ago (https://www.themotte.org/post/842/culture-war-roundup-for-the-week/181915?context=8#context)
That said I think I go a bit further - I think Left/right as a meaningful political divide is going to either go away or simply transform into pro/anti regime/establishment, because neither of them can offer anything which actually helps people deal with the problems they're facing in their daily lives. Trump is just the early foreshadowing of that realignment.
SteveKirk
10hr ago
I saw the imgur front page the other day (because someone couldn't see a catbox link), and it's literally worse than reddit. Then you go to funnyjunk or iFunny and it's all zoomer holocaust jokes. Same with the old forums, resetera vs rpgcodex(?) etc.
Social media is totally pillarized at this point, but it seems obvious to me that the leftist ones reach far more people. It's just that the leftist extremism has gone way too overboard to actually help the Democrats; they're trying to run a "we're normal, they're weird" campaign, and their entire youth wing is posting "glory to the martyrs for stomping magat colonizer babies to protect trans kids" memes.
I'm honestly surprised he's still around considering everything, still more that he's getting that kind of work. Read the first two nights dawn books in elementary school, and the Commonwealth trilogy when it first came out.
Probably should get around to rereading and finishing the former, but it's harder to justify burning through a pile of doorstops in a weekend the way you could as a kid.
Quantumfreakonomics
10hr ago
After the assasination of Franz Ferdinand, but before the outbreak of war, the Russian ambassador to Serbia, Nicholas Hartwig, died suddenly while visiting the Austro-Hungarian embassy in Belgrade. The official explaination was that he died of a heart attack.
One house on my street had a single sign that just said "Kamela". Every single one of the others had multiple signs, banners, and flags. One at the intersection had a big banner of trump snarling with some slogan about the face of stupidity, racism, and fascism. Most others also got updated What This House Believes signs with the new firmware.
They all popped up within a week of the Kamelanomicon being opened.
Suspect I'm on a list for not having one. With the neighborhood going 80D-15R it's pretty easy to spot the dissidents.
orthoxerox
If you can read this, you're using a custom theme
11hr ago
Xiaomi something something, 6 liters, mechanical controls (Alec Watson convinced me I didn't need a fancier one).
hooser
11hr ago
Thanks for sharing the study, it is really very good! Reading it was a Sunday well-spent.
The conclusions that the authors reach have a lot of nuance, and help explain both why so many people have negative impressions of NPs while others have positive impressions: the variability of the productivity[1] within each profession dwarfs the difference between the average NP and the average doctor.
The other useful estimate from the study: randomly pick an NP and a Doctor working for VA emergency department; 6 out of 10 times, the Doctor is more productive, 4 out of 10 times, the NP is.
I understand that VA hospitals have trouble attracting talented doctors, though I assume that they have similar problems attracting talent in other professions, NPs in particular.
If I were in charge of VA, I would make a rule that any doctor who got their license in any OECD country can work unsupervised (provisional on training on HIPPA or whatever other US-specific medical laws). Then get a whole bunch of H1 Visas for any doctor who wants to come work for VA for five years.
[1] "productivity" was operationalized as the total cost of care (negatively coded), including the cost for any avoidable hospitalization due to screwing up, which makes sense in the VA emergency department.
FormerPothead
11hr ago
I just blew through 1,000 page Exodus by Peter F Hamilton. I’m pretty mixed on PFH. I loved Commonweath but I’ve tried and fail to get into his others. I’m taking a stab at Nights Dawn but that’s besides the point
I thought Exodus was great. His best work in quite some time. The universe, pacing, major plot lines - all great. Good characters. The dude is really really imaginative.
The book is actually contract work where it’s and in-universe tie in novel with a new sci fi RPG that’s in development but some legit ex-BioWare guys. I’m very skeptical that the game won’t be woke slop since it’s being published by WOTC.
All this is to say that I hope more people read this book and it has some success. PFH is legit and doesn’t seem to have gone performatively woke even if he has been bullied into no longer including sex scenes in his stories.
 George_E_Hale
insufferable blowhard
11hr ago
George_E_Hale
insufferable blowhard
11hr ago
men grow cold as girls grow old / and we all lose our charms in the end
The trade-off of being a very beautiful woman is the extremely brief shelf-life. Female beauty, at least in terms of "hotness," is very ephemeral.
pigeonburger
11hr ago
My friends and I were speculating the other day how this could be improved within the current constraints of our public health system, we landed on a mix of telehealth and licensed practitionners (could be NPs) who specialise in making observations (and auscultations, etc...) for doctors to extend the amount of ailments that can diagnosed by a remote doctor.
My work insurance has as one of its perks free access to a telehealth service and it's shocking how convenient it is compared to going through the public health pipeline, when it is able to help. I'm sure it's convenient to the doctors who work through that system too.
 Lazuli
11hr ago
Lazuli
11hr ago
Invest. Make your money work for you. Start by putting your money in a high-yield savings account.
MollieTheMare
11hr ago
Low-calorie does limit your options. Not necessarily for dipping and in no particular order:
- Malt Vinegar, possibly with some amount of "brown sauce." If it works for fish and chips, it probably works with just chips
- Tomato Chutney or salsa, especially with larger home fries
- Mustard, stone ground or whole grain. According to the totally unbiased National Mustard Museum, superior in every way to using ketchup. Particularly for the calorie conscious.
- Nutritional yeast. I guess a topping not a sauce, but still another option to complement fries. IMO, needs salt too. Low calorie and low sodium sounds very miserable. Kind of a funky cheesy flavor with way fewer calories than cheese sauce.
- Hot sauce. Frank's RedHot reminds me the most of using ketchup. Melinda's is available pretty broadly, and has a bunch of flavors of varying spiciness.
- Gochujang. Depending on what you're having the fries with, but surprisingly versatile as a sauce for something so strongly associated with Korian food.
- Crema. Can be lower calorie if made with yogurt or fat free sour cream, less tasty that way of course.
Personally, I don't worry too much about the calories from a table spoon of sauce. I typically go for Ketchup, BBQ, or 1:1 fry sauce (as apposed to 2:1 of Mayochup, as a concession that mayo does have appreciable calories, even at the table spoon level). If squeezed from a fine tip condiment food service bottle, you can "cover" a pretty large area with relatively little sauce.
ulyssessword
12hr ago
I think I want to build self contained mini factories.
Take a look at this: https://www.themotte.org/images/17324829035101736.webp
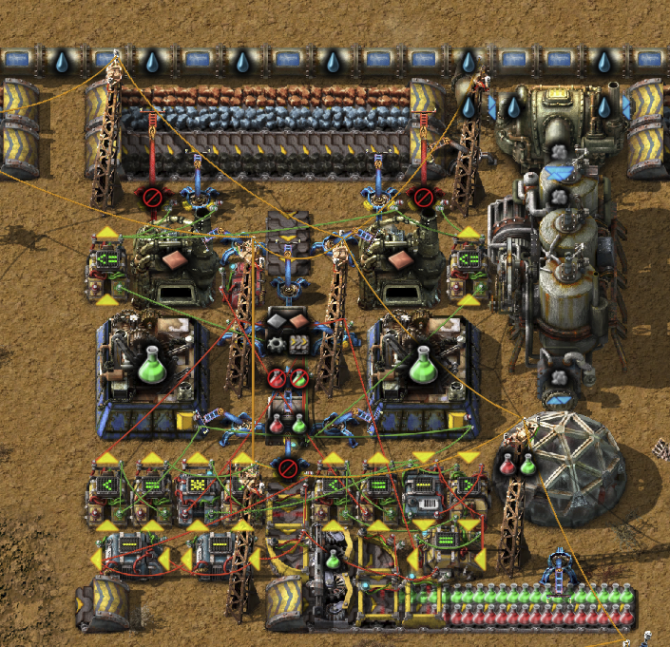{kind=link}
I'm making red/green research from ore, coal, and water. It's moderately impractical, but still cool.
0eNrtW11u3DYQvkqgx0IbrH6oH6MN4Jf0qUDRBkiAwFhotbSXiFZSKa1TI/ABeo+erCfpDCWtpBUlkbLXToG+JGOK83E4nF+a/mZskyPNOUtL4+qbweIsLYyrz9+Mgt2lUYJjaXSgxpVR8igt8oyXqy1NSuPRNFi6o38aV9ajKZlelDQ6rGh6x1LamWw/3pgGTUtWMlotJH542KTHw5ZyQDMbhJzl1DCNPCtgcpYiNgK8JabxYFyRt+QRFz5jt2fYnWl2Z4bdnWZ3Z9jJNDuZYfem2b0Zdn+a3Z9hD6fZgxn2YJo9nGG3rGl+az0HsJ4BmLM8a8Z2rDnbs2Zs12qt7wjewu94Bv9X7jbqB3Co4F07xmlcfQUbLB9yBMmOZX5ETx2u5C5YyVu0UmvTZwFk1DWHO5Lhetq4nhKur4xLtOQNlHFdLdxQW14lPdhrbXnVcC1lXF9HD7atjOtp4Tra8qrpwdWWVw2XaHh2OB9DWDri2La3YCFvyULqHhlonWygjat2AqFqIvJGapDW9bZHnlK+YmlBeQnfxrEGW7ZsGXTrfduMJVLEU2Lp4wUyuNbpDnTHjlDvJTCfs3iVZ8lE8RaM7Lx1tiRL71b7CCxrN7F9p4NnGlC7ljxLNlu6j+5ZxnFSzHh8ZOWmoOXmliWAAlVnyY8U5h8Lej42FKn109uoKCdkacJrqHYSRBXX7e3xJC9Uzk39fUJiPEtXGUfF/3GMElgPBtOMH6AyR/Uc8ohHJSrG+Em4WlOUnxDiLM/B4JQxbmRb81S35o+pTOZXjq8dMQe4UiMONI0uvLzRhaoaDP5rxuGuNUPGKcKNxAy33eGOxgwy0Qrk2LJUyDEagaz1yNnVIBv4thOMhTjRzk+g3FvGCzje855XqDhPolJ0vNhKlxH21RZZn2nnn7/+NrATrgrnkY77dGICLH8AmY4pWBTPDpsqXV7dRklBQdFSzXRPrhJlUjXkpJphBJPrqqgmFH26Z3zzJnlHI776uqc0UbIqHDgKpUptdBAaNBDtDqJzbvVxtE2oHp7TwWvTSGXvWQoWX8cJPVS3g9omkU6I0MAiHaw2akfHMjtEeJqrImY0jekqj+IvetBeB9rvRNg7VpSw9eXAfgcYe/a6frxnvDwKxuYCSrjT6lrXqm66doWuBY6SRA8QEna0iDnLK58wfvtZVq26jm69gBcbg6J4KqvQFE1xV2UP8zR8ClE49zxAzSjpUz9eBWf6eWfIA0xr1EUJ/ru6hXI1imXXZk3MlaEoV0JeN0DJkLQLj6Hux0Ld96d8vx9G4z0tJkohsVMZTKB6huHUGYZaSfiU0y+SheuALcnDy9Jwp+xZlojJ2pTeio/3XmMWTtrcGRUFPWwTBhXrIYr3gLeyxxskRH4cS+LlBswfW9XaqDmNdpuvGf8C4O0YzoDKNWXFnu7Urfs9Kq0GU+f6aGDcbcSayEi1XIMIL1OebrdKusqTAerHekc33jwlsLzvW/9aLbAQVzuKOpoZ7BU2pZ9k7EHzOL0p4TXYPOL2Sli/OE8S4qOYdsh2VFSw0/XxUwoxaXW8vPzCKFnJWgtvbBPgTZhIOipNLfE03c+fcz/NDOiMwASaMTX8P6a2ytNL/Kd0RJ4z78/s+0M/YoRrqXHLS4DZ5mJZReCtl11afBdqo5uaE8KZsAlN4I8V8KD/GmIvPZYPxmP/TYLaVvWPUe/uiVzkGEfuUqYL33eG2QPapLTEgCIW5NjfiH2bxh2nNK1juuysRx+HtIvbl168d0PTW9q79NKSy5yX3fupkHnZZceSx8tKIS9nLiHD5RKETpyK0odyjwUEgKqJLQ9bbUEYcVbuDxR1OBW53LnI1eKcBS/N3ECh7MLdFRRh9PkyCARRfUH3g9Ecmj6OtoWciTzkqUq+mqU6evnhONqdinuxX0R5+q8ULPLsfVMz3u+dZOISrXzsv0ZZdd2PT/4LR6OxkODphoSwq7z5054JEL2G/jmcf7XY+eX68bUsK3gNy1oaO68l9fhiE2uEWFJNBwsvkdUs8JIqP7+Cepr2UDczNcOYCtt2PIm2UxfM7sgb4PWCh6HWkvdjvqUbcZxqMU/1ClU55NgSn5mrMGdjzTSA9PT8xRfU/shpOro6Jq+g44leQlXLoxByPeu8fvYUjHz8+bNP9AsoT/M2/RkLKL8tA4o8YeX0tb8/ELOqJ2fNX+3+ujntnMOGq8kJvZWrWf+N6FDNL1en+upPT8Mp83spcUN97b6iuIH2EzOraxMyRPVH6y2W0iPkwNaseTTj8wU7mLP72+kuRtb9mk/tncjz3hp/eta7mmvNO+hPo71ZoP4nCG1NrGZ96u396Y+fFJHV855l6yErP/JpgXVD/ZJHPvPFjHaN2fOxH8Vv7y736+Ib9JuvoCIE/+zYJjGJZ5Ib87PjmLbpWqaLNOnQAdJhRYed8bAdd9ctDnyGcd+0kbZNy4Sm2kLaAdr1Wtpbmw7SMGRCgBQ0TDVJPR9pz25oG8cFZtjSBNciQUsDpqA7+xI01NyCJi0+fjYhiYhx3CPIiXshYYVT067pVftF6GYchiwcdyraRjnrcZjvCRlg6ITp4X79er6LNBEyeKhn+Mc90UFDu8grcFA/MO5UtJhTjztICxz4jDpE2kfZoCWoaQdp5EUVNPv1nVYG/M+E3C9ov0MHLR3gXgLcI1gPK+lBPAxo/qDYxC6Ugq0b5M3vv/7y5sBinm2jAnPwPZixcCXi2aEbhsS1XNu2IKP/CxDwYT4=
bonsaii
12hr ago
Even for something that happens every week at an average hospital, if you go from 10 residents to 40 you're going from residents who have trained on it 25 times to residents who may have only done it 6 times.
ChickenOverlord
12hr ago
The fact that the YouTube comments for Kirby's Air Ride: Item Bounce haven't been closed yet is proof that YouTube doesn't have complete control over ideology on their platform.
MadMonzer
Temporarily embarrassed liberal elite
12hr ago
The pro-life movement is funded and staffed by fundamentalists, and they wrote the legislation. By and large, the pro-life movement do support an exception for sufficiently dangerous-to-the-mother pregnancies . They don't support an exception for non-viable fetuses, which forms part of a pattern where pro-life Christians (particularly Catholics) support heroic intervention to keep non-viable babies like Charlie Gard alive for as long as possible, as well as their opposition to withdrawing treatment from effectively non-viable adults like Terri Schiavo. I think pro-life Christians are consistent in their attitude to these cases and that it reflects their religious beliefs, but I profoundly disagree with them.
I don't know why Ken Paxton chose to noisily go after a mother who wanted to abort a non-viable fetus, but he did. I hope the median general election voter applies condign punishment, but given the nature of Texas politics I doubt it. My best guess is that Paxton is positioning himself to run for governor, and the main obstacle is a Texas Republican primary in which the median voter is well to the right of Donald Trump. One weakness of the American electoral system is that in a 60-40 state like Texas it tends to elect a government that represents the median Republican, not the median voter. And given that almost 40% of Americans claim to be young-earth creationists when polled, I don't think that fundamentalists are going to be a small minority of Texas Republicans.
HB3058 doesn't cover non-viable fetuses, it clarifies two particular cases where there is a genuine threat to the life of the mother (as opposed to the fake threat to the mother's continued fertility that Cox's lawyers tried to use to work around the lack of an exception for non-viable fetuses). Unlike danger-to-mother cases where there is clearly a desire to produce workable rules that allow a reasonable margin of discretion to the doctor treating an emergency case without opening a loophole the size of a barn door, I see no movement from the pro-life right in the US on this point.
Throwaway05
12hr ago
It's called the art and science of medicine for a reason, in psych it can be pretty evident to the lay man, in other specialties it's less but still present. This means experience, heuristics, gestalts, they lead doctors astray yes, but for a lot of things we don't have good guidelines or understanding.
Importantly, doctors can be sued - this causes all kinds of problems but it does serve as a feedback mechanism that assess for problems and gives patients recourse.
Let me give a specific example of how this happens, sticking with psych because it's more interesting than me mumbling about open vs lap vs conservative appendix management.
Most people are aware of Bipolar disorder, at least superficially. Lots of people say "I have mood swings" and tell that to healthcare workers with less training, these people dutifully write down Bipolar in the chart. Or they say "you ever like have mood swings and be unable to sleep?" Gets the diagnosis. Someone who actually has Bipolar 1 with a manic episode barely sleeps for a week of more, does illegal things, or spends ALL of their money in the bank account and all kinds of other stuff. The diagnosis is serious and life limiting without treatment. The medications are also serious - most patients get antipsychotics these days which increase all cause mortality. They are worth it if you actually have the disease. Put undertrained staff give the dx to people who don't have it and then suddenly...
NPs also do things like mix benzos and stimulants, put people with depression or anxiety on antipsychotics which will result in an early death....just all kinds of ridiculous stuff.
The skill ceiling in psych (and medicine) is very high, but if you don't work in healthcare you'll (hopefully) never see it come into play. Most medical work isn't your quick annual physical with your doctor but for many patients (especially young ones) that's all you see.
As for the second point, no the issue is that physician salaries are less than 10 percent of healthcare spending, and it's been decreasing every year. Cutting doctor salaries does not solve the problem and introduces all kinds of new problems.
Likewise NPs don't save money because they do more unnecessary testing and over consult, which drains the specialists and slows down care.
 urquan
12hr ago
urquan
12hr ago
I'm sure there have been some converts, but I don't doubt that there have been enough progressive young tech workers joining the field to more than balance them.
There are not official gradations of lawyers, but it's widely understood that there are (specialties aside) bad, okay, good and fantastic lawyers, and the public has a good idea where specific levels of quality are found. They know that is all you can get is a mall lawyer, your chances are much lower (for the same quality of case) than if you could hire a prestigious law firm. Doctors associations cling to the idea that (specialties aside) doctors are essentially fungible, and this is even more explicit in countries where a public system assigns doctors to the public. Of course, this is preposterous to the public, you don't have to be a doctor yourself to spot when one is particularly good or not. Anyone with a bit of life experience has seen lazy doctors, doctors who don't listen to them and give them an obviously bad diagnosis because of it, and on the other side doctors who spotted something from hard to read symptoms. My wife recently got assigned by our healthcare system to a shifty clinic in a bad neighborhood where the clinic also advertises "natural remedy treatments" alongside having actual licensed doctors, and to our system that's good enough: to them she needed to be assigned to a clinic, any clinic, they're all as good as one another, and if she wants to switch she gets shoved to the back of the line and likely will be without an assigned clinic for 5 years. And on the opposite side, an optometrist going above and beyond speculating about the reason for me having an uveitis led to me having an auto-immune disease diagnosed and my quality of life improved dramatically.
Know exactly what kind of person you are.
More options
Context Copy link